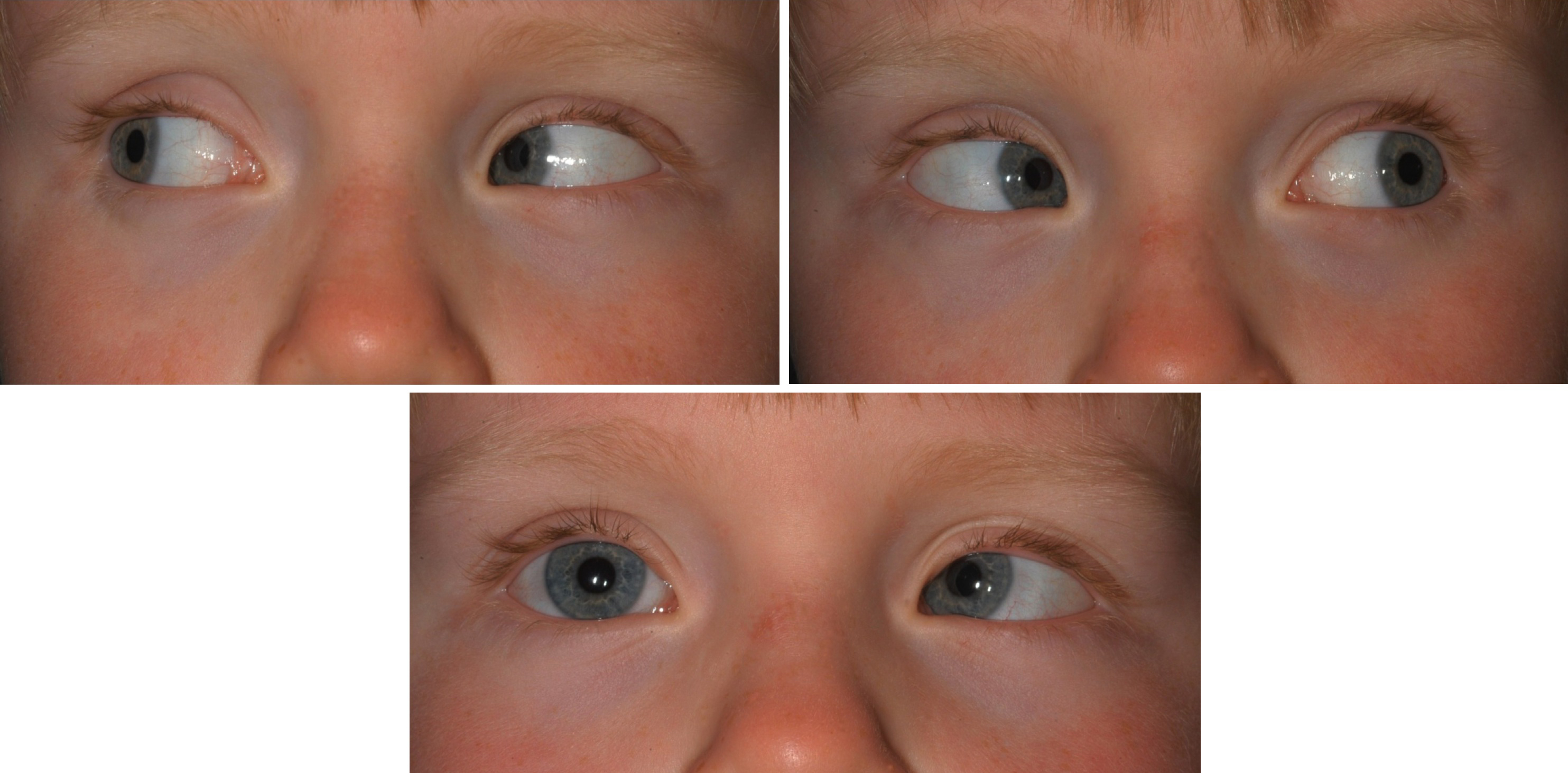
What is a deviated gaze?
A deviated gaze is an abnormal movement of the eyes. It is often found as a symptom for subdural hematoma or some people may have it from birth. A deviated gaze can result from several complications.
Does gaze deviation predict stroke outcome?
Conclusions: Gaze deviation is a good predictor of large artery occlusion and if present can positively predict hyperacute interventions. Incorporating their use in prehospital and increasing their weightage in a 'modified' NIHSS can be used as a strategy to reduce ‘the time of onset of symptoms to treatment’ in hyperacute stroke.
What is the difference between forced deviation and forced gaze paresis?
gaze is abnormal in one or both eyes, but forced deviation or total gaze paresis is not present. Forced deviation , or total gaze paresis is not overcome by the oculocephalic maneuver. 3
What is non conjugate lateral gaze deviation?
Non-conjugate lateral gaze deviation This refers to a situation where an unconscious patient, at rest, has some sort of fixed gaze devition of both eyes in different directions.
What causes eye deviation?
Causes. The causes of eye misalignment are various, and sometimes unknown. Potential causes include high farsightedness, thyroid eye disease, cataract, eye injuries, myasthenia gravis, cranial nerve palsies, and in some patients it may be caused by brain or birth problems.
What is eye deviation?
Strabismus is a condition in which the eyes do not point in the same direction. It can also be referred to as a tropia or squint.
What is gaze deviation in stroke?
It is a well-known phenomenon that some patients with acute left or right hemisphere stroke show a deviation of the eyes (Prévost's sign) and head to one side. Here we investigated whether both right- and left-sided brain lesions may cause this deviation.
How do you assess gaze deviation?
0:451:4203 - mNIHSS - Gaze - YouTubeYouTubeStart of suggested clipEnd of suggested clipIn this case we see the eyes moving in the direction opposite that of head movement as. The eyeMoreIn this case we see the eyes moving in the direction opposite that of head movement as. The eye movements appeared to be unrestricted with the ocular cephalic maneuver this item would be scored zero.
What is gaze asymmetry?
Gaze asymmetry measurements screen for potential muscle imbalance or misalignment of the eyes (strabismus). Corneal reflexes are recorded on the “targets” shown below the picture of your child's eyes, as well as in the list of criteria. The screener detects whether the eyes are moving together properly.
What is angle of deviation in eye?
The “angle” of deviation, or the “angle” of squint is usually defined as the angle between the visual axis of the fixating eye and the visual axis of the deviating eye. This definition is approximately correct numerically only for horizontal deviations measured at 6 meters.
What causes left gaze deviation in stroke?
An acute, destructive lesion involving the right fron- tal lobe will cause a left hemiparesis and leftward gaze palsy. The eyes, "driven" by the remaining normal left hemisphere, will be deviated to the right (i.e., the eyes look toward the side of the lesion).
Can eye deviation be cured?
Treatment for strabismus may include eyeglasses, prisms, vision therapy, or eye muscle surgery. If detected and treated early, strabismus can often be corrected with excellent results. People with strabismus have several treatment options to improve eye alignment and coordination.
What causes gaze preference?
Common causes include strokes for horizontal gaze palsies, midbrain lesions (usually infarcts and tumors) for vertical gaze palsies, and progressive supranuclear palsy for downward gaze palsies. Treat the underlying disorder.
What is lateral deviation of the eyes?
Objective: Ocular lateral deviation (OLD) is a conjugate, ipsilesional, horizontal ocular deviation associated with brief (3-5 s) closing of the eyes, commonly linked to the lateral medullary syndrome (LMS). There is limited information regarding OLD in patients with the acute vestibular syndrome (AVS).
Definitions
Humans have a large field of vision but a very small area of high spatial resolution acuity, subserved by the fovea. The purposes of having eye movements are to maintain constant foveation of an object of interest or to foveate a target quickly.
Symptoms
Most patients with conjugate gaze abnormalities offer only vague visual complaints such as blurriness or dizziness when looking up or down. Those with downgaze palsies may complain that they are unable to read, go down steps, or eat, but such patients are usually unaware that the problem stems from an inability to look down.
Examination
Smooth pursuit can be tested at the bedside by having the patient follow a slowly moving target with both eyes. The slow phase of OKN and suppression of the VOR by visual fixation are two other ocular motor functions related to smooth pursuit eye movements.
Approach
One method for distinguishing supranuclear conjugate gaze disorders is to divide them into those that cause primarily horizontal vs vertical defects, although there is considerable overlap ( Boxes 16.1–16.4 ).
Saccades
The major cortical control of horizontal saccadic eye movements, especially intentional ones, lies in the frontal eye fields (Brodmann area 8). Each hemisphere has a frontal eye field located in the posterior portion of the second frontal gyrus and the adjacent part of the precentral gyrus and sulcus ( Fig. 16.1 ).
Smooth Pursuit
Two descending parallel pathways mediate smooth pursuit ( Fig. 16.3 ). In one, cortical signals arise from the occipito-temporal-parietal junction in Brodmann areas 19, 37, and 39 (area V5, see Fig. 9.7B ), which are homologous to monkey areas MT (middle temporal) and MST (medial superior temporal).
Vestibuloocular Reflex and Optokinetic Nystagmus
Fibers mediating the VOR arise from the posterior, anterior, and horizontal semicircular canals, synapse in the vestibular nuclei, travel rostrally via the MLF (with two additional upward or “antigravity” pathways for the anterior canals), and pass through but do not synapse in the caudal portion of the PPRF; then finally horizontal canal afferents arrive and synapse at the sixth nerve nucleus, and anterior and posterior canal afferents proceed to the third and fourth nuclei.
Why do the police use HGN?
The manual used to train all officers in the United States, the NHTSA manual, contains the instructions and strict testing protocol for this test because it is believed to be strongly correlated with alcohol impairment at or above a .08% blood alcohol level. The HGN instructions from the manual read as follows:
Horizontal Gaze Nystagmus
The Horizontal Gaze Nystagmus (HGN) Field Sobriety Test checks your eyes for involuntary jerking as you gaze to the side. The test begins by the police officer placing the tested person in the instructional stance where the feet are placed together and the arms are kept to the side.
Horizontal Gaze Nystagmus (HGN) Field Sobriety Test Administration
According to NHTSA, the testing Deputy must provide the instructions for the test to the suspect in a standardized manner covering specific elements.
Qualification
According to NHTSA “Prior to the administration of the HGN, the eyes are checked for equal tracking (can they follow an object together) and equal pupil size. If the eyes do not track together, or if the pupils are noticeably unequal in size, the chance of medical disorders or injuries causing the nystagmus is present” (P.
Lack of Smooth Pursuit
According to NHTSA, “Check the suspects left eye by moving the stimulus to your right. Move the stimulus smoothly, at a speed that requires approximately two seconds to bring the suspects eye as far to the side as it can go. While moving the stimulus look at the suspect’s eye and determine whether it is able to pursue smoothly.
Distinct Nystagmus at Maximum Deviation
NHTSA says, “After you have checked both eyes for lack of smooth pursuit, check the eyes for distinct nystagmus at maximum deviation beginning with the suspects left eye. Simply move the object to the suspects left side until the eye has gone as far to the side as possible.
Onset of Nystagmus Prior to 45 Degrees
NHTSA says, “Next, check for onset of nystagmus prior to 45 degrees. Start moving the stimulus toward the right (suspects left eye) at a speed that would take approximately four seconds for the stimulus to reach the edge of the suspects shoulder. Watch the eye carefully for any sign of jerking.