A positive straight leg raise test usually indicates S1 or L5 root irritation. Sensitivity is about 91%, and specificity is 26%. Pain that does not increase with dorsiflexion or neck flexion may indicate a lesion in the lumbosacral, sacroiliac, or hamstring area. Pain on the opposite side could indicate a large spac-occupying lesion. 1,17,37
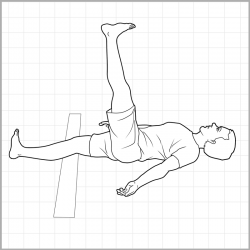
How should I do straight leg raises?
- Lay flat on your back, legs straight
- Engage your abdominals to help protect your lower back
- Place your hands by your hips for added support
- Exhale as you lift your leg into the air
- Lift until you form a 90 degree bend at your hips
- Slowly lower returning to start
What does a negative straight leg raise test mean?
A negative test suggests a likely different cause for back pain. [citation needed] A positive straight leg test reproduces radiating leg pain. If it only causes back pain, then the test is negative. Because this is often misunderstood, it is prudent to add a statement of clarification.
What is SLR positive?
What is the SLR?
- Reserve Should be Excluded, but Maybe Not Treasuries. The purpose of all this regulation is to make banks safer by strengthening their solvency and liquidity.
- Non-Renewal Implication 1: Banks May Hold Fewer Treasuries. ...
- Implication 2: Front End Rates Will Go Lower. ...
What is a positive SLR?
- Primary care provider
- Orthopedic surgeon
- Neurologist
- Neurosurgeon
- Sport's medicine specialist
- The nurse
- Physiotherapist
- Chiropractor
What is a negative straight leg raise?
A negative test suggests a likely different cause for back pain. A positive straight leg test reproduces radiating leg pain. If it only causes back pain, then the test is negative.
What is normal SLR?
Ideally, normative SLR range of motion in healthy, asymptomatic individuals could be used for comparisons to testing in clinical populations. Unfortunately, when used as a neurodynamic test, normal SLR range of motion is highly variable, averaging from 40° to 85° [1,3,6,9].
What does 90 90 straight leg raise test?
A clinical test used to identify hamstring muscle tightness. The patient lies supine with the hips and knees flexed to 90º and grasps behind both of his or her thighs to stabilise the hip joints, then actively extends each knee in turn.
Is straight leg raise test positive in spinal stenosis?
Most patients with a true positive straight leg raising sign complain of excruciating sciatica-like pain in the elevated leg at 30 to 40 degrees of elevation. This sign is usually absent in patients with lumbar stenosis.
How accurate is straight leg raise test?
A positive straight leg raise test usually indicates S1 or L5 root irritation. Sensitivity is about 91%, and specificity is 26%. Pain that does not increase with dorsiflexion or neck flexion may indicate a lesion in the lumbosacral, sacroiliac, or hamstring area.
How do you do a straight leg test?
0:472:47Straight Leg Raise or Lasègue's Test for Lumbar Radiculopathy - YouTubeYouTubeStart of suggested clipEnd of suggested clipYou would start by assessing the unaffected leg. First then flex your patients leg at the hip jointMoreYou would start by assessing the unaffected leg. First then flex your patients leg at the hip joint whilst keeping the knee in a fully extended position.
What is considered severe spinal stenosis?
Symptoms of Severe Spinal Stenosis When spinal stenosis progresses to the severe stage, that means there has been substantial narrowing of the spinal canal. This can occur due to several different factors, but is most commonly caused by degeneration of the discs, vertebrae and spinal ligaments.
How many mm is severe spinal stenosis?
A sagittal diameter of 12 mm is considered as narrow (relative stenosis) and a diameter of 10 mm or less is considered a severely narrowed (absolute stenosis) according to Verbiest.
What is stenosis of L4 and L5?
Most commonly, it involves the L4 slipping over the L5 vertebra. It is usually treated with the same non-surgical (“conservative”) and surgical methods as lumbar spinal stenosis. Degenerative scoliosis occurs most frequently in the lower back and more commonly affects people aged 65 and older.
What is a straight leg raise test?
Most often, the straight leg raise test is used to assess the function of the quadriceps muscle and its attachment to the shin bone. A disruption of the. When someone has a condition such as a torn quadriceps tendon or a patella fracture, they are generally unable to perform this maneuver.
What does a positive leg raise test mean?
A positive straight leg raise test usually indicates S1 or L5 root irritation.
What does a negative straight leg test mean?
One may also ask, what does a negative straight leg test mean? A negative test suggests a likely different cause for back pain. A positive straight leg test reproduces radiating leg pain. If it only causes back pain, then the test is negative.
What does a positive leg raise test mean?
A positive straight leg raise test usually indicates S1 or L5 root irritation.
What does a negative straight leg test mean?
Similarly, what does a negative straight leg test mean? A negative test suggests a likely different cause for back pain. A positive straight leg test reproduces radiating leg pain. If it only causes back pain, then the test is negative. For example, "Straight leg test is positive on the left, reproducing the patient's radiating leg symptoms."
What are the stages of SLR?
The six SLR stages: 1 SLR is negative: a minor disc protrusion/internal derangement is still possible. 2 SLR is painful, not limited: the protrusion cannot be large. 3 Painful arc on SLR: again, this must be a small easily reducible internal derangement. 4 Painful, limited, without neurological deficit: a somewhat larger protrusion, interfering with mobility, not with conduction. 5 Painful, limited, with neurological deficit: severe compression, not only of the dural sleeve about the nerve root, but also of the parenchyma. Both mobility and conduction are disturbed. 6 Negative (no limitation, no pain) but with neurological deficit. The patient has had a sciatica for some time. Now thepain gets even worse for minutes or hours or even days, after which rather suddenly the pain disappears completely and SLR becomes negative again. This is an ischaemic root atrophy: the protrusion is maximal, the compression is so severe that the nerve root has become ischaemic. Stretching it causes no protective reflex anymore and SLR ceases to hurt. There is motor and sensory deficit, possibly with loss of knee or ankle jerk. The patient has become symptomatically better but anatomically worse.
Is SLR negative after manipulation?
After the next manipulation, SLR become s negative, although there is no full reduction yet. Some movements in standing may still be painful. We continue our manipulative strategy, but from now on the positive movements in standing become our new control test criterion.
Is SLR negative or positive?
Negative ( no limitation, no pain) but with neurological deficit. The patient has had a sciatica for some time. Now thepain gets even worse for minutes or hours or even days, after which rather suddenly the pain disappears completely and SLR becomes negative again. This is an ischaemic root atrophy: the protrusion is maximal, the compression is so severe that the nerve root has become ischaemic. Stretching it causes no protective reflex anymore and SLR ceases to hurt. There is motor and sensory deficit, possibly with loss of knee or ankle jerk. The patient has become symptomatically better but anatomically worse.
Is SLR a root test?
The SLR is not only a root test but also a dural test. Just like neck flexion stretches the dura upwards, SLR stretches it downwards. Actually, we can state that any considerable limitation of dural mobility results in a limited or painful SLR.
What does a straight leg raise test show?
from readings, The straight leg raise test is used to assess for the impingement of a nerve root from a herniated disc or from a space-occupying lesion by stretching that root. ... A positive straight leg raise test usually indicates S1 or L5 root irritation. Sensitivity is about 91%, and specificity is 26%. I back has issues in this area mine runs L1-S1. In addition my neck C1–6 has issues. I feel your pain if you have it.
What does "positive SLR" mean?
Thanks for the question.Positive SLR means neural involvement, which indicates S1 or L5 nerve root irritation. It also helps to analyse the severity of disc lesion.
Why is the sciatic nerve stretched up?
It means that the sciatic nerve which has the origin from the lumbosacral roots is stretched up due to a disc prolapse or rarely a tumour and is very sensitive . Hence the patient needs rest and further investigation like an MRI scan
Can lumbar disc herniation be positive?
This test can be positive in a variety of conditions, though lumbar disc herniation is the most common.
What is a straight leg raise?
The straight leg raise (SLR) or Lasegue's sign is a widely used test to assess the sciatic nerve in cases of back pain. Although widely used, the test has limited diagnostic accuracy when diagnosing herniated discs.
How many degrees of flexion do you need to press your leg?
Leg press for 0 to 45 degrees of flexion.
How to do wall sit isometrics?
First, the patient can voluntarily set the quadriceps muscle once he or she reaches the maximum knee flexion angle, which is typically between 30 and 45 degrees. This contraction and knee flexion position are held until muscle fatigue occurs. In a second modification, designed to promote a stronger vastus medialis obliquus contraction, the patient performs a hip adduction contraction by squeezing a ball between the distal thighs. In a third variation, the patient holds dumbbell weights in the hands to increase body weight, which promotes an even a stronger quadriceps contraction. The patient can shift their body weight over the involved side to simulate a single-leg contraction, or perform the wall-sit on just one leg.
What is an ASLR test?
The active straight leg raise test (ASLR) examines the ability of the patient to transfer load through the pelvis in supine lying and has been validated for reliability, sensitivity, and specificity for pelvic girdle pain (Mens et al 1999, 2001, 2002 ). It can also be used to identify nonoptimal stabilization strategies for load transfer through the pelvis in the supine position. The supine patient is asked to lift the extended leg 20 cm and to note any effort difference between the left and right leg (does one leg seem heavier or harder to lift). This is not a test for pain and the patient should only score the effort. The strategy used to stabilize the lumbopelvic region during this task is observed ( Fig. 40.4 ). The leg should flex at the hip joint and the pelvis should not rotate, sidebend, flex, or extend relative to the lumbar spine. The rib cage should not draw in excessively (overactivation of the external oblique muscles), nor should the lower ribs flare out excessively (overactivation of the internal oblique muscles), nor should the abdomen bulge (breath holding – Valsalva). The pelvis is then compressed passively and the ASLR is repeated; any change in effort is noted. The location of the compression can be varied (anterior, posterior, oblique) to determine where more compression (force closure) is needed for optimal load transfer ( Fig. 40.5) ( Lee 2004 ).
When to start toe raises after meniscal transplant?
At weeks 3 to 4, weight-bearing exercises are begun. Toe raises for gastrocnemius-soleus strengthening, wall-sits, and minisquats for quadriceps strengthening are initiated when patients are 50% weight bearing. Wall-sits ( Fig. 25-9) and minisquats ( Fig. 25-10) are begun at 5 to 6 postoperative weeks after meniscal transplantation. These activities should be limited from 0 to 60 degrees of flexion to protect the posterior horn of the meniscus.
Where does hip flexion occur during SLR?
As hip flexion goes through 35°, movement occurs proximal to the ala of the sacrum, and during the next 35° the movement is at the intervertebral foramen itself.
What position should a patient be in when flexing their hip?
The patient should be in a supine position. The physician flexes the patient’s hip with the patient's knee extended until the patient complains of pain or tightness in the back or the back of the leg. At this point, the physician brings the leg back down until the patient feels no pain.
What is a straight leg raise?
The straight leg raise is a passive test. Each leg is tested individually with the normal leg being tested first. When performing the SLR test, the patient is positioned in supine without a pillow under his/her head, the hip medially rotated and adducted, and the knee extended.
What is a straight raise test?
The leg is raised straight raise test when performed when the subject is placed supine, the therapist grasps the ankle and lifts the leg straight up, while stabilises the same anterior superior iliac spine. If the leg cannot be raised beyond 80degrees the hamstrings is considered tight.
What is the SLR test for ankle dorsiflexion?
Inclusion of ankle dorsiflexion in the SLR is documented as Lasegue's test or Bragard's test. Inclusion of great toe extension in the SLR (instead of ankle dorsiflexion) is documented as Sicard's Test.
What is a modified leg raise test?
Modifications to the Straight Leg Raise test can be used to stress different peripheral nerves to a greater degree; these are referred to as SLR tests with a particular nerve bias.
What does it mean when your hip is hurting at 30 degrees?
Pain at less than 30 degrees of hip flexion might indicate acute spondyloithesis, gluteal abscess, disc protrusion or extrusion, tumor of the buttock, acute dural inflammation, a malingering patient, or the sign of the buttock.
How does a clinician lift a patient's leg?
The clinician lifts the patient's leg by the posterior ankle while keeping the knee in a fully extended position. The clinician continues to lift the patient's leg by flexing at the hip until the patient complains of pain or tightness in the back or back of the leg.
Does a positive lumbar disc test increase specificity?
Combining positive test results increased the specificity of physical tests, but few studies presented data on test combinations. The authors of the meta analysis conclude that When used in isolation, current evidence indicates poor diagnostic performance of most physical tests used to identify lumbar disc herniation.